
Keren Landman is a senior reporter covering public health, emerging infectious diseases, the health workforce, and health justice at Vox. Keren is trained as a physician, researcher, and epidemiologist and has served as a disease detective at the US Centers for Disease Control and Prevention.
When I was in training to be an infectious disease doctor, there was a running joke that if a hospital team didn’t want to review the chart, they could just consult infectious diseases and we’d do it for them.
It got laughs largely because it felt so true. A core function of infectious disease doctors — often abbreviated as “ID” in medical circles — is to diagnose and guide treatment (and, sometimes, prevention) of a variety of conditions ranging from pneumonia to bone infections to HIV to malaria. That requires a lot of highly cognitive work, including taking notoriously detailed histories and, yes, conducting notoriously thorough reviews of medical records.
That kind of work takes a lot of time. Most ID doctors have completed not only the three years of internal medicine residency training most hospitalists have done, but also an additional two to three years of specialty ID fellowship training. Fortunately, it also pays less than many other medical professions.
It’s tough but rewarding work. However, there’s a persistent shortage of these critical physicians, and relatively few medical school graduates are pursuing this career.
On November 30, when thousands of US doctors continuing their medical training learned where they had matched for fellowship, one-quarter of US ID training positions went unfilled. That feels like particularly dire news at this moment, with every season seeming to bring its own unprecedented infectious challenges, and our overburdened public health and health care systems sounding increasingly loud alarms about the need for more resources.
For a profession so demonstrably critical to the nation’s health — one whose most senior practitioner in the US — Anthony Fauci — is influential enough to have inspired entire lines of merch — the news came with a distinct sense of whiplash. How could so many prospective trainees shun a field whose physicians and scientists produced the Covid-19 vaccine, guided mpox treatment, and are currently helping overwhelmed hospitals dig out from under the triple-demic?
Even if you never need the services of an ID doctor, it’s worth understanding what’s at the root of this trend and why it matters.
ID doctors fight infections and antibiotic overuse
The key role of most infectious disease doctors is figuring out whether a patient has an infection and how best to treat it.
Sometimes, that means starting an antibiotic, but often, it means choosing to stop or not start antibiotics, changing intravenous antibiotics to ones people take by mouth, or switching from a “big gun” antibiotic to one less likely to lead to a resistant germ. These physicians also often lead infection control efforts in facilities; that is, they help prevent patients and visitors from contracting infections while inside the hospital.
These individual decisions add up to greatly improved outcomes. Studies have shown infectious disease consultation saves lives in patients with fungal or bacterial bloodstream infections, organ transplants, and a variety of other conditions. Deploying these physicians can also save money and prevent antibiotic overuse.
The judicious use of antibiotics is a key countermeasure against the emergence of antibiotic-resistant superbugs, which the WHO has declared a global emergency. As institutional leaders in antibiotic stewardship, ID doctors often play an important role in helping reduce unnecessary or overly broad antibiotic use.
Other types of physicians and health professionals can perform some of the functions infectious disease doctors do. More than 1,700 infectious diseases pharmacists play critical roles in guiding safe and effective antibiotic use, as do many nurse practitioners and physician assistants, and many internists (that is, general adult medicine doctors) became experts in treating HIV well before specialty HIV training existed.
But whatever their professional category, people need pretty extensive training to do the job of an infectious diseases practitioner right, said Wendy Armstrong, an ID doctor who co-directs Emory’s ID fellowship. “Anybody can prescribe antibiotics — maybe not well, but anybody can,” she said.
When ID doctor training programs go unfilled, that means there are fewer people guaranteed to get the training to do this work right.
The ID doctor shortage is especially bad in rural America
Despite there being a shortage of ID doctors, demand for them is rising, said Carlos del Rio, the president of the Infectious Diseases Society of America.
New drugs for treating immune system disorders and cancers and the increasing availability of organ transplantation (and the immunosuppressive drugs it requires) are resulting in rising numbers of immunosuppressed Americans while advances in critical care mean extremely sick people can be kept alive for longer. And while international travel remains slowed due to the pandemic, travelers continue to return from abroad with infections infrequently seen in the US.
All of these trends increase the likelihood that general practitioners will encounter patients with infections they don’t know how to treat but that are squarely in most ID specialists’ wheelhouses.
In 2017, 80 percent of US counties did not have even one ID doctor, and about 208 million citizens lived in counties where inadequate ID expertise was available.
More recent models from the federal Health Resources and Services Administration (HRSA) suggest the US is currently short about 240 ID doctors, and will be short far more — about 7 percent nationwide — by 2035. These models also suggest the shortfall is entirely concentrated in rural areas, with those areas having only 17 percent of the specialists they need.
T. Neil Ku, an ID doctor in Billings, Montana, said that while rural places may have abundant recreation opportunities in the outdoors, “that can only go so far” when it comes to attracting ID providers to practice.
Fewer providers means a heavier workload for the ones that do opt for a rural practice, making those settings even less appealing, he said. Additionally, due in part to longstanding inequities and political polarization, rural America has higher rates of public distrust for ID specialists and public health.
That has led to politically driven rollbacks in public health protections, and in many rural places, a sense of practicing in a hostile environment. That means that as far as ID provider access goes, the future holds only worse health inequities for rural residents than they already face.
The HRSA projections may underestimate the actual shortages, as they do not account for the possibility that pandemic-related provider strain may lead more currently practicing professionals to leave the profession early due to burnout.
Regardless, it’s not looking like supply is going to meet demand: In 2023, only 328 physicians will enter ID training programs — only a few more than in 2017. That’s a significant drop from an uptick in trainees earlier in the pandemic, as you can see in the chart below.
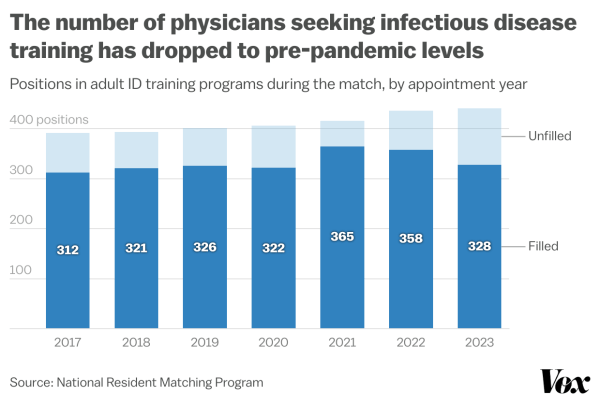
It’s not clear whether that uptick represented a temporary increase in interest due to the “Fauci effect” — in other words, his function has a role model — or whether this year’s numbers represent a true crash in interest.
Brad Cutrell, an ID doctor who directs the fellowship program at the University of Texas Southwestern Medical Center, thinks it’s a little of both. “The two prior years were an illusory blip where it seemed [the] pandemic might increase interest,” he wrote me.
Why? A big reason is that there hasn’t been meaningful change in the structural issues that discourage so many doctors from choosing to specialize in ID.
The US is short of ID doctors because hospitals don’t get paid for people to think
One of the biggest barriers to having more ID doctors is pay.
Everyone I spoke with noted that ID doctors don’t merely get paid less than other specialists, they get paid less than doctors with less training. According to Association of American Medical Colleges data and a 2017 IDSA survey, ID doctors who care for patients make around $175,000 to $215,000 annually — which doesn’t go as far as you’d think given most US doctors’ are hundreds of thousands of dollars in educational debt. It’s also less than half of what some other specialties earn.
Armstrong said she hears a common refrain from residents considering specialty training: The additional years of training required for the ID specialty is just not worth it to them financially.
Quality of life is also an important factor. In a Medscape survey, ID doctors were among the most burned out, and cited high burdens of bureaucratic tasks, long hours, and a lack of respect as important contributors.
It doesn’t help that medical residents (that is, physicians who’ve graduated medical school but are still in training) mostly encounter ID practitioners grinding through late hours at the hospital, said Armstrong. “Exposure is important,” she said. ID doctors can also work in less frantic settings, but prospective trainees don’t often see that.
Plus, there’s some brain drain going on too: The pharmaceutical industry has helped suck countless doctors away from clinical ID practice to work on vaccine and drug development with higher salaries, said del Rio.
These problems persist because the profession is not seen as a profit driver for hospitals, said Ku. Hospitals’ main source of income is insurance company reimbursements for care — and insurance companies pay much less for cognitive work like history-taking and chart reviews than they do for hands-on work like surgeries. “We spend 99 percent of our time thinking, and unfortunately, thinking doesn’t pay as well,” said Ku.
So even though ID doctors add immense value to teams by improving patient outcomes, they’re underpaid because those outcomes don’t translate into big dollars. “We’re a specialty people love to consult,” but organizations don’t like to pay for, said Ku, “because we don’t generate the revenue compared to all the other specialties.”
Fixes are far off
We’re a long way from seeing meaningful changes in compensation or working conditions for infectious disease doctors. But there are some ideas to fill the gaps.
One involves increasing the number of international medical graduates in ID training programs. Non-US citizens who completed US residency training after graduating from medical school abroad currently comprise 26 percent of new ID trainees.
But the training pipeline is full of disincentivizes for non-US citizens. While fellowship directors might want to hire these trainees, funding for training slots often comes from federal programs that have citizenship requirements, said Armstrong. Furthermore, trainees who intend to conduct research as part of their careers face a dead end when they enter the professional world: The NIH “starter” grants that kick off researchers’ careers have a US citizenship requirement, which makes them off-limits to many international graduates.
“We are losing an incredibly promising generation of physician-scientists — incredible, incredible candidates, very smart minds — who cannot make it in this country because they are not eligible for NIH dollars,” said Armstrong. Del Rio said this issue is one IDSA is actively advocating to change.
It’s not only ID training programs that are facing challenges. Pediatric ID programs only filled half of their available training slots. And other fields that have been and will continue to be first-line during public health emergencies are also seeing waning interest: Seven percent fewer emergency medicine training spots were filled this year than last year.
Ku wasn’t sure exactly what he’d do to fix the system’s problems, but any viable solution would need to restore some of what initially drew so many ID practitioners to the field. “ID as a specialty has to be sustainable,” Ku said. Doctors need to feel joy and passion for what they do every day, “without feeling like they’re a hamster in a little wheel that just keeps going on and on and on and on.”
Sourse: vox.com






